GastroSAM: Rethinking Rehydration for Malnourished Children
GastroSAM: Rethinking Rehydration for Malnourished Children
January 2026
Challenging Long-Standing Guidelines
For over 25 years, treatment guidelines for children with severe acute malnutrition (SAM) and severe dehydration from gastroenteritis have differed significantly from those for well-nourished children. Because SAM affects heart and kidney function, rapid IV rehydration has been feared to overwhelm these fragile organs. As a result, the World Health Organization (WHO) recommended the use of a low-sodium oral rehydration solution (ORS), and restricted IV fluids to cases of shock under strict medical supervision.
Despite these precautions, hospital data from several African countries have continued to show high mortality from dehydration among children with SAM. The conservative approach in the rehydration guidelines has largely been based on expert opinion rather than strong clinical evidence.

Study Design
The GASTROSAM trial, a randomized controlled study conducted in close collaboration among Médecins Sans Frontières (MSF), Imperial College London, and University College London (UCL), evaluated the safety of both rapid and slow IV rehydration in 272 children with SAM and severe dehydration in Niger, Nigeria, Uganda and Kenya.
Read the full study here.
272 children - aged 6 months to 12 years - presented at the facilities were randomised into one of 3 rehydration strategies:

Findings That Challenge the Status Quo
Key takeaways
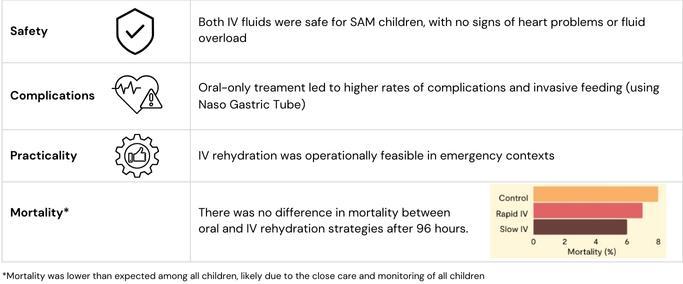
These findings provide the first robust clinical evidence that children with SAM can safely receive IV fluids using protocols similar to those for non-malnourished children. In response, the WHO has expressed openness to revisiting its recommendations.
What This Means for Field Care
These results could lead to changes in global guidelines, enabling simplification of protocols for IV rehydration of SAM children, aligning with those for non-malnourished children - highly needed in contexts like Sub-Saharan Africa.
Close monitoring and quality bedside care were likely key factors in lowering paediatric mortality, as demonstrated in this trial. Equipping frontline health workers with the knowledge and skills to systematically monitor vital signs, recognize early clinical deterioration, and respond promptly, especially in settings with limited monitoring resources, must be a priority.